About the Device
 USAGE INSTRUCTIONS
USAGE INSTRUCTIONS
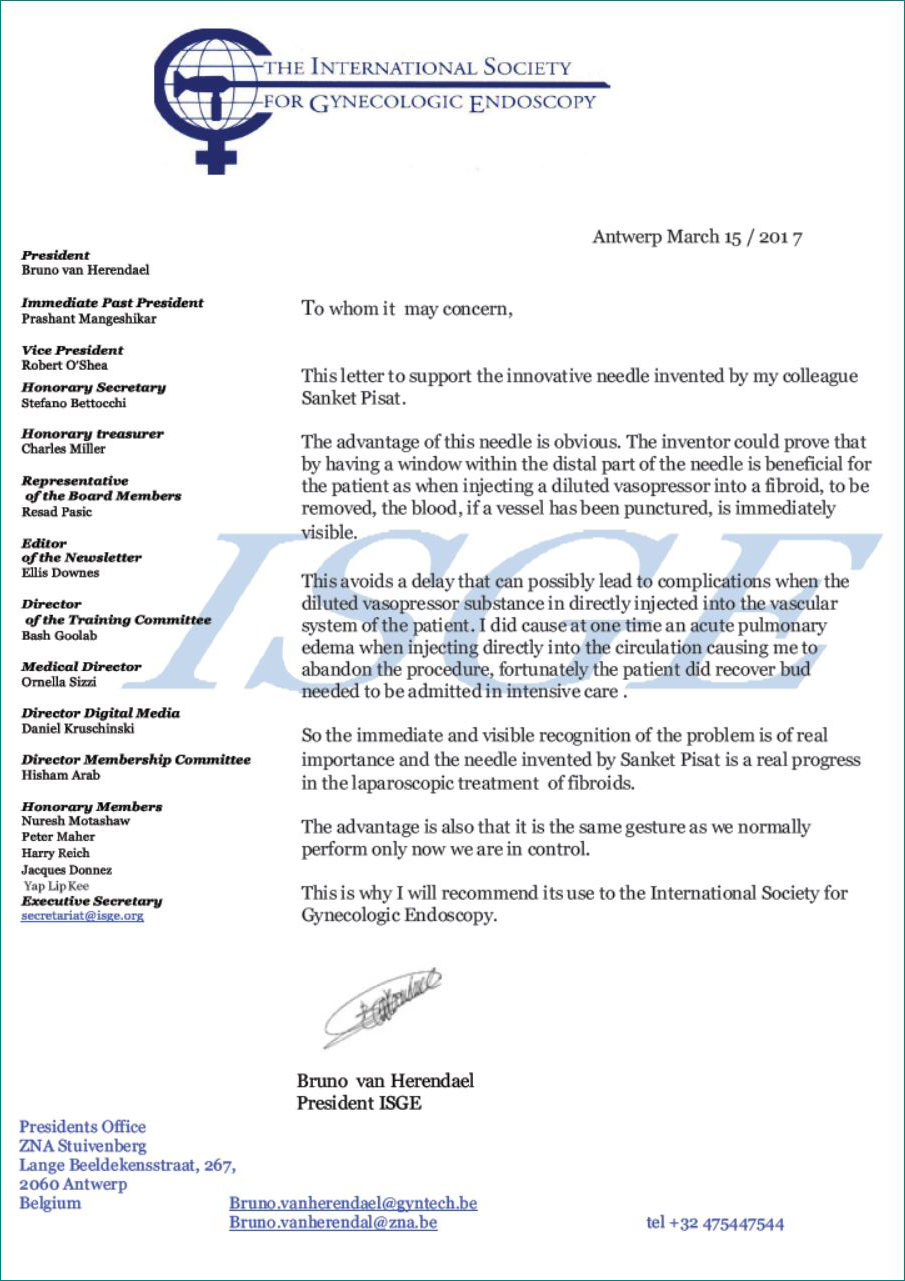
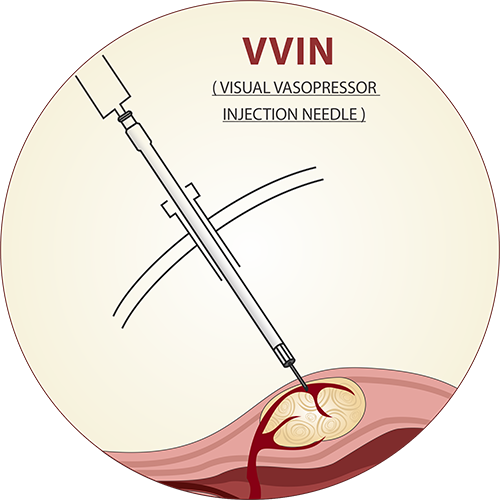
When myomectomy is performed by laparotomy, the surgeon always aspirates into the syringe after the needle has entered the myoma capsule. In case the tip of the needle is in a blood vessel, the clear solution within the syringe, or within the transparent hub of the needle is stained with blood, and the surgeon immediately withdraws and repositions the needle, thereby avoiding an intravascular injection.
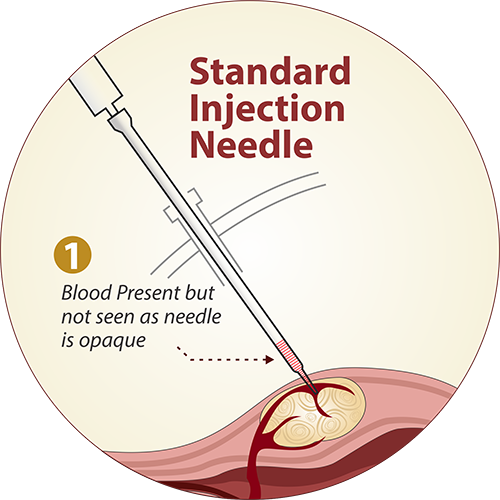
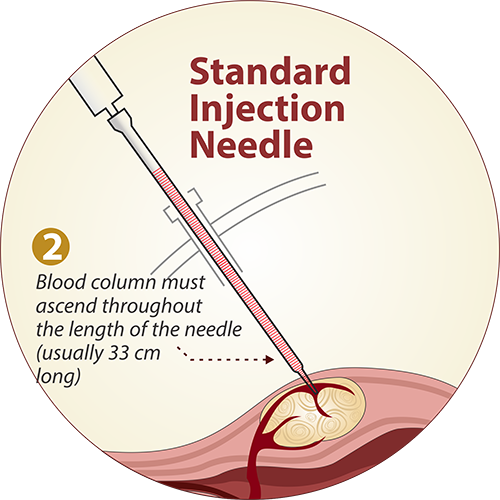
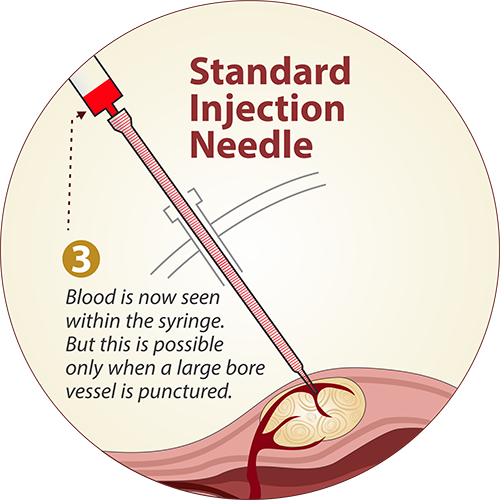
In laparoscopic surgery, the length of the needle used is 33 cm. Even if the surgeon were to puncture a blood vessel within the myoma and aspirate, the blood column would not rise to a distance of 33 cm, high enough to stain the fluid in the syringe red. Most vessels in the myoma capsule are thin walled venous channels rather than arterial ones. Hence, the negative pressure caused by aspiration would temporarily empty the blood vessel (albeit momentarily), and the total volume of blood aspirated into the injection needle would never be sufficiently large so as to create a blood column sufficiently high to stain the fluid in the syringe red.

DETAILED DESIGN OF THE VVIN
The VVIN is a 33 cm long and 5mm wide hollow bore metallic instrument, quite similar to the 5 mm laparoscopic needle that is used for infiltrating vasoconstrictor solution during laparoscopic myomectomy. At the proximal end of the instrument, which remains outside the abdomen, is a hub that attaches to a standard disposable syringe. At the terminal or business end which is inserted into the abdomen, the VVIN has a detachable, disposable tip which can be fixed on to the shaft by a screw locking mechanism.

The Visual Vasopressor Injection Needle
THE VVIN TIP
The disposable VVIN tip has a plastic hub and a terminal metallic needle tip. The plastic hub is transparent, 1 cm long, and has a hollow central cylinder measuring 2 mm in diameter. The lumen of this hollow cylinder is continuous with the lumen of a 2.5 cm long metallic needle tip which is attached to the terminal end of the instrument. The detachable terminal portion makes the instrument easy to clean. This avoids the need and cost of a single use disposable instrument, as the metallic shaft can be sterilized and re-used.
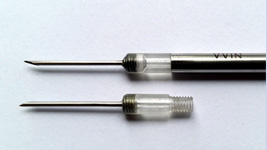
Detachable tip of the VVIN
USING THE VVIN
The VVIN along with the disposable tip is first flushed with dilute vasopressin solution to remove the air column within the VVIN. The VVIN is then inserted through any standard 5 mm port into the abdominal cavity.
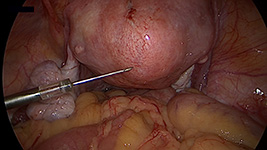
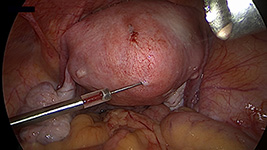
The VVIN before insertion into fibroid
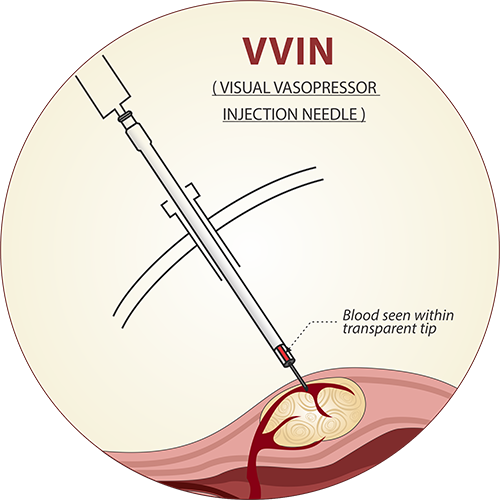
A suitable site over the myoma is chosen as per the surgeon’s preference and the VVIN inserted into the fibroid capsule, so as to lie in the sub-capsular plane. Using a 20 ml syringe, negative pressure is applied. If the tip of the needle has inadvertently punctured the lumen of a blood vessel over the fibroid, the cylindrical column within the plastic hub of the VVIN immediately shows a blood stained aspirate- a positive aspiration test.
The VVIN before insertion into fibroid
Alternatively, if the needle is not in a vessel lumen, the aspiration test shows clear fluid
The concept of minimum aspirate quantity
To determine exactly how much volume of blood is required to be aspirated to yield a positive aspiration test, a simple experiment was performed. A container was filled with a dilute solution of methylene blue dye. Three needles were used: a standard 5mm laparoscopic aspiration needle (A), a standard 3mm laparoscopic aspiration needle (B) and a VVIN (C). A 10ml syringe was connected to each of these 3 needles and aspiration of methylene blue solution was done till blue coloured fluid was seen at the tip of the syringe in (A) and (B), and at the transparent hub of the VVIN in (C). The total quantity of aspirate in each case was collected and measured with a micro pipette.
It was observed that
- With a standard 5 mm aspiration needle, approximately 0.8 ml of solution was required to demonstrate a positive aspiration test.
- This quantity was reduced to 0.35 ml with a 3 mm aspirat
- The minimum aspirate quantity was markedly low (0.03ml) for a VVIN.

Minimum Aspirate Quantity
Thus, even an inadvertent puncture of a blood vessel that is of very small calibre can be detected using a VVIN, which would quite likely be missed using the other two needles. The VVIN is thus about 27 times more sensitive than a regular injection needle, and can detect blood at a quantity of LESS THAN ONE SINGLE DROP
USAGE INSTRUCTIONS